

Sessions
Conference Agenda
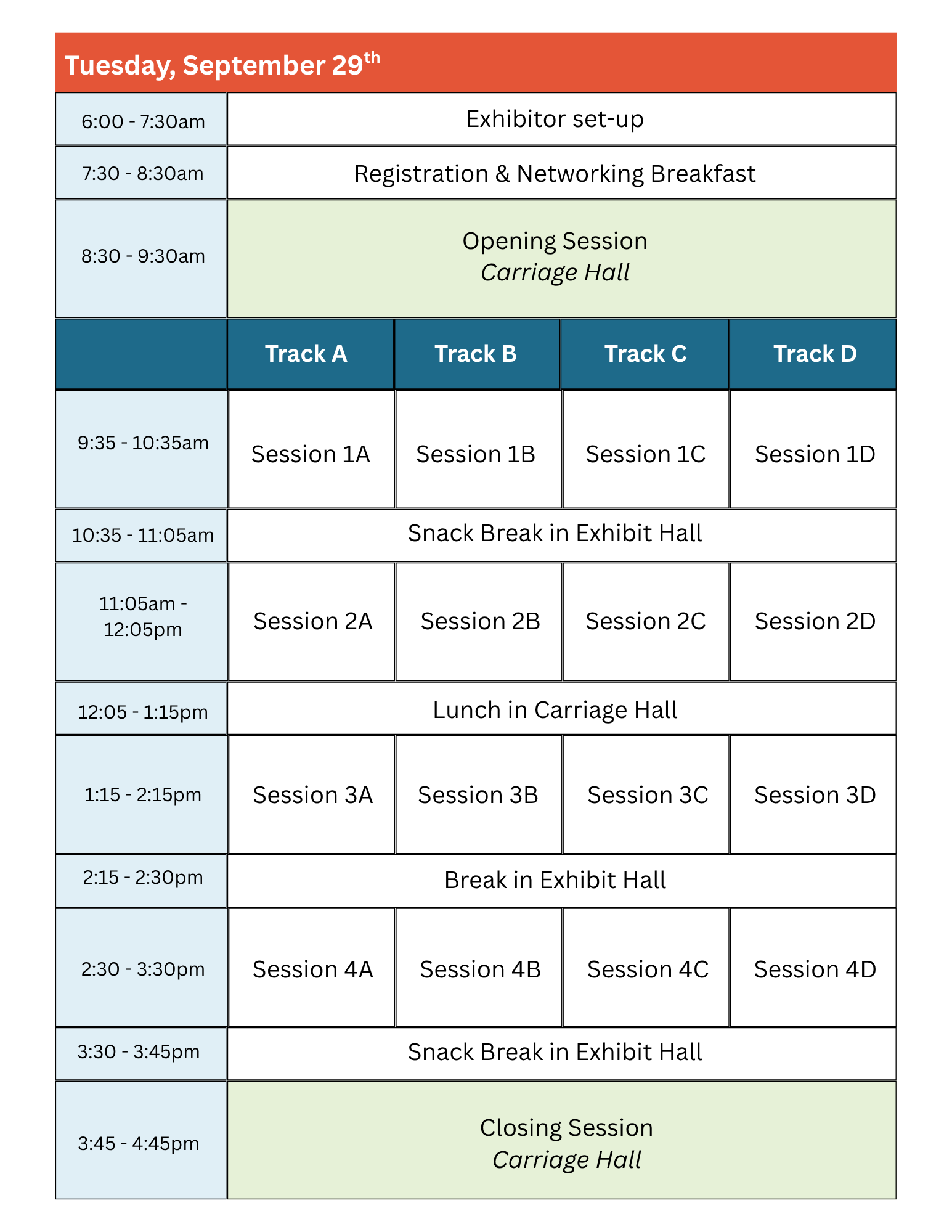
2025 Sessions and Agenda


Click images to view PDFs!
Click images to view PDFs!